When Pregnancy Meets Chronic Disease: The Hidden Challenge in Maternal Health
Until now, throughout most of human history, the priority in maternal health care has been obvious – make sure that the mother and the infant survive childbirth. Huge strides have been made in achieving this goal. However, another silent revolution is taking place in antenatal wards worldwide – something that current health care systems are just beginning to recognise.
Nowadays, more and more women come into pregnancy already burdened with chronic diseases such as hypertension, diabetes, obesity or depression before pregnancy. Pregnancy, far from being a neutral factor in the course of these diseases, intensifies them, reveals their hidden vulnerabilities and poses additional threats both to the mother and the infant. Maternal health of the 21st century is, in spite of any official stance of health systems, a matter of non-communicable diseases.
The Burden No One Counted
NCDs are the greatest health problem in the world currently. As per the World Health Organization, in 2021, over 43 million people died of NCDs accounting for three-quarters of non-pandemic deaths around the world [1]. Another area where less attention has been paid to NCDs is their link with pregnancy.
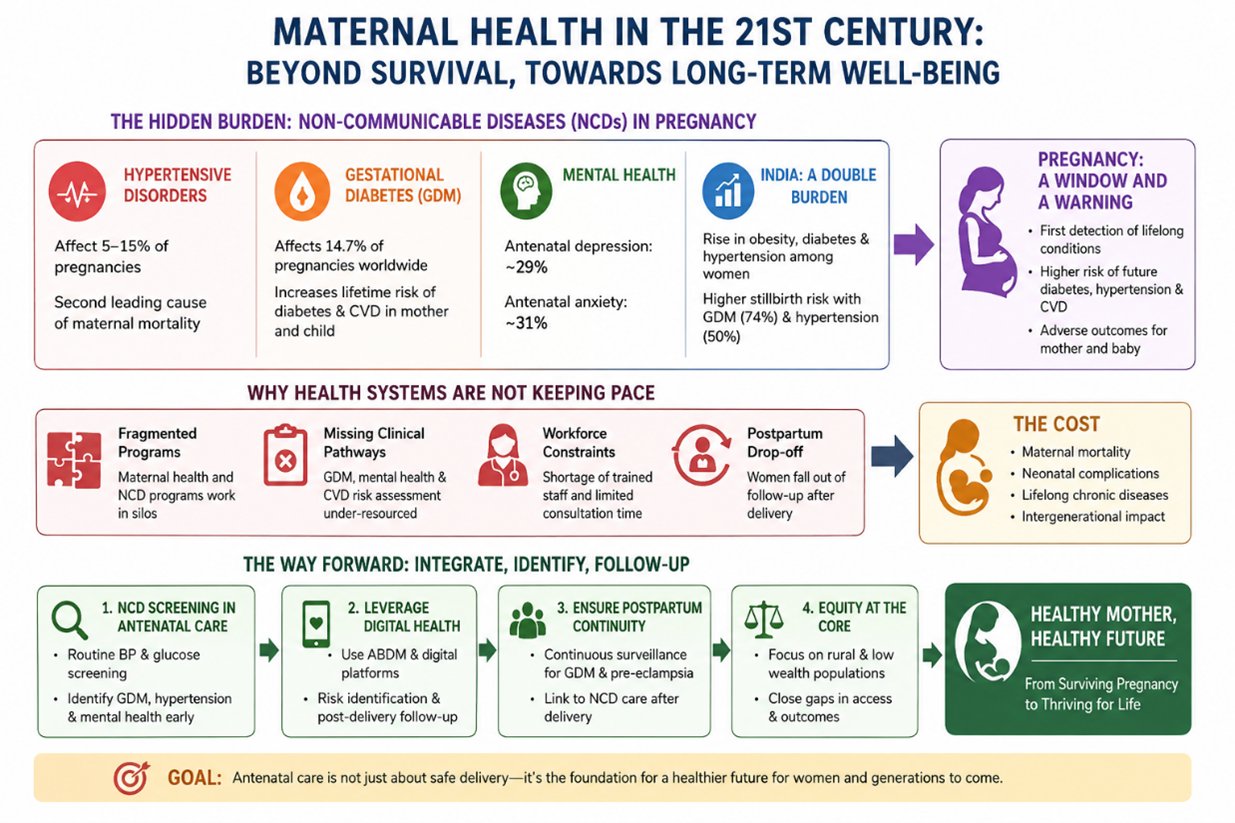
The hypertensive conditions in pregnancy include gestational hypertension, pre-eclampsia, and eclampsia. They affect 5-15% of all pregnancies and represent the second largest cause of maternal mortality across the globe [2]. While the age-standardized prevalence rate of such diseases decreased in various regions, total cases increased by 15.87% from 1990 to 2021.
The story of gestational diabetes mellitus (GDM) is no less frightening. According to the International Diabetes Federation, its prevalence was estimated to be 14.7% of all pregnancies worldwide by 2021. Women who have GDM are exposed to higher lifetime risks of type 2 diabetes, and the risks of obesity, metabolic syndrome, and cardiovascular disease for their offspring in adult life are also increased. One case of GDM can trigger an intergenerational pattern of chronic diseases.
Finally, mental well-being needs to be considered. In 2024, an umbrella review reported the pooled prevalence of antenatal depression to be 29%, and that of antenatal anxiety to be 31% among studies carried out during the COVID-19 era [6]. In pre-COVID-19 times, perinatal depression was estimated to affect between 10 and 20% of women worldwide [7]. This is not infrequent complication. This is a prevalent problem that is often not screened at all.
India: A Double Burden Taking Shape
There have been many successes for the country in improving maternal health with reduction in maternal mortality, increased institutional deliveries and antenatal care through the National Health Mission. However, there is another problem that is arising in the backdrop of all this progress.
Data from NFHS-5 (2019-21) indicated that gestational diabetes mellitus was a factor that increased the likelihood of stillbirth by 74% (odds ratio 1.74) while hypertension increased it by 50% (AOR 1.50) [8]. An observational study conducted in 2025 and published in Cureus journal found that urbanization, increased obesity and maternal age played a critical role in GDM and hypertensive disorders among pregnant women in India.
According to a study done in PLOS One using data from NFHS-4 and NFHS-5, there is an increase in the prevalence of diabetes and hypertension among reproductive-aged women from 2015–16 to 2019-21 with poor treatment and control, especially in low socio-economic quintiles. There was also confirmation of the presence of significant gaps in the treatment of hypertension among reproductive-age women, especially those residing in rural areas.
India has the issue of a double burden within maternal health itself – the burden of anaemia and malnutrition, and now, an increased risk of metabolic and cardiovascular disease, which was not envisaged by the antenatal programs.
Pregnancy as a Window — and a Warning
It is one area in which pregnancy brings the unique feature of having guaranteed repeat encounters with the healthcare system for nine months on end. To any healthcare system that takes its role in NCD prevention seriously, it should be noted that such an opportunity currently goes unrealized.
The incidence of GDM increases the lifetime risk of developing type 2 diabetes significantly. Similarly, a woman who suffers from pre-eclampsia will face a 2.4 times higher risk of developing hypertension within ten years after giving birth. It is possible that antenatal visits are the first time a woman becomes aware of a condition she will have for the rest of her life. Additionally, maternal hyperglycaemia, hypertension, and obesity each increase the likelihood of preterm birth, low birth weight, and macrosomia.
Why Health Systems Are Not Keeping Pace
Antenatal care in most low- and middle-income countries is designed around obstetric monitoring: blood pressure, haemoglobin, fetal position. Clinical pathways for GDM screening, mental health assessment, and cardiovascular risk stratification either do not exist or are under-resourced.
Structural fragmentation makes this worse. Maternal health and NCD programmes operate through separate verticals — separate supply chains, reporting systems, and staff training. A woman diagnosed with gestational hypertension may receive care during pregnancy and then fall entirely outside the NCD follow-up system postpartum, precisely when longitudinal tracking is most needed. Workforce constraints compound the problem, with mental health screening tools and cardiovascular counselling requiring trained staff and consultation time that peripheral facilities rarely have.
The Way Forward
Certain guiding principles can be adhered to in implementing this idea. For instance, antenatal care should be rethought and considered as an avenue for chronic disease screening. Currently, blood glucose and blood pressure tests are carried out during antenatal sessions in India's NHM. However, there is still a lack of follow-up actions for after delivery. Patients with GDM and pre-eclampsia must receive continuous surveillance after birth.
The second principle relates to the use of digital health. There is considerable potential in utilizing platforms created under Ayushman Bharat Digital Mission to identify risk factors for NCDs in patients' medical history and carry out post-delivery follow-up. It has been proved that such an approach is feasible and effective based on mobile apps used to screen antenatal depression.
Finally, equity has to be designed into integration efforts. Patients who belong to low wealth quintiles and rural populations experience the biggest burden of NCDs as well as the lowest access to specialized care. An integration strategy not considering them will increase the existing disparities.
Conclusion
Safedelivery will be crucial. However, if the policies regarding the health ofpregnant women end here, then the policies will ultimately fail women. GDMindicates the future onset of diabetes. Pre-eclampsia indicates the developmentof cardiovascular disease. Untreated perinatal depression will affect themother and child for years to come. There is no ambiguity regarding this issue.
Indiaand other developing countries have reached this stage in history where all thecomponents necessary for this change, including antenatal facilities, digitalhealthcare services, and awareness about NCDs, coincide. What needs to be seenis whether the policies make the linkages between these components before thecost — maternal mortality rate, neonatal disorders, and lifelong chronic diseases— becomes too high to reverse.
Healthcarepolicy for mothers in the modern world does not only consist of making surethat the women survive the pregnancy period.
References
1. WHO/SDG Target 3.4 NCD Data. (2021). NCDs killed over 43 million people in 2021. https://www.who.int/data/gho/data/themes/topics/sdg-target-3_4-noncommunicable-diseases-and-mental-health
2. Wang X, et al. (2025). Global burden of maternal hypertensive disorder from 1990 to 2021. medRxiv preprint. https://www.medrxiv.org/content/10.1101/2025.04.01.25325061.full.pdf
3. Tang Z, et al. (2025). Global, regional, and national trends in hypertensive disorders of pregnancy (1990–2021). Frontiers in Global Women's Health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12098623/
4. Berhe T, et al. (2024). Double burden of gestational diabetes and pregnancy-induced hypertension in Ethiopia. PLOS One. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11446441/
5. MedScriptum. (2025). Global epidemiology of diabetes and WHO's recommendations for diabetes in pregnancy. https://medscriptum.org/en/diabetes-epidemiology/
6. Sriskandarajah P, et al. (2024). Global prevalence of perinatal depression and anxiety during the COVID-19 pandemic: An umbrella review. Acta Obstetricia et Gynecologica Scandinavica. https://pmc.ncbi.nlm.nih.gov/articles/PMC10823409/
7. Abadiga M, et al. (2021). Prevalence and Associated Factors of Depression among Pregnant Mothers. PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8195633/
8. Yadav J, et al. (2025). Maternal metabolic health conditions and risk of stillbirth in India: NFHS-5. PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12239305/
9. Revathi J, Meena TS, Pavithra M. (2025). Prevalence of Medical Disorders During Pregnancy in India. Cureus. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12276767/
10. Tripathy JP, et al. (2024). Correlates of diabetes and hypertension in India: NFHS-4 and NFHS-5. PLOS One. https://journals.plos.org/plosone/article?id=10.1371%2Fjournal.pone.0305223
11. Kapoor N, et al. (2023). Hypertension treatment cascade among women of reproductive age in India: NFHS-5. The Lancet Regional Health — Southeast Asia. https://www.thelancet.com/journals/lansea/article/PIIS2772-3682(23)00131-2/fulltext
12. BMC Pregnancy and Childbirth. (2024). Antenatal depressive symptoms across trimesters using mobile app-based screening. https://bmcpregnancychildbirth.biomedcentral.com/articles/10.1186/s12884-024-06680-z